
Every time he sees an AED, Marvin A. Wayne, MD, FACEP, FAAEM, FAHA, is reminded of its history. That’s because he was part of its history.
“Think of the thousands of people who have been saved by the AED worldwide,” says Wayne, medical program director for Washington’s Whatcom County EMS and assistant clinical professor at the University of Washington. “You can get some discussion of who invented the defibrillator, who developed penicillin, and so many other medical discoveries and developments. But nobody knows who invented and developed the AED.“
Wayne’s part in the story started in Oregon in the early 1970s, when physicians Arch Diack, MD, and W. Stanley Welborn, MD, joined forces with engineer Robert Rullman to brainstorm ways to bring defibrillation to patients in the field.
At that point out-of-hospital defibrillation was in its infancy. Few EMS systems had the capability, and defibrillators weren’t designed for mobile use. Public access defibrillation didn’t exist yet.
“In the early 1970s a very select number of prehospital units were carrying defibrillators,“ says Wayne. “They were big and clunky, but they worked. There was nothing for the public and nothing readily available to grab off the shelf or wall.“
The thought that Diack and others had was to create a device that could hang on the wall like a fire extinguisher and be easily accessible and usable by the public.
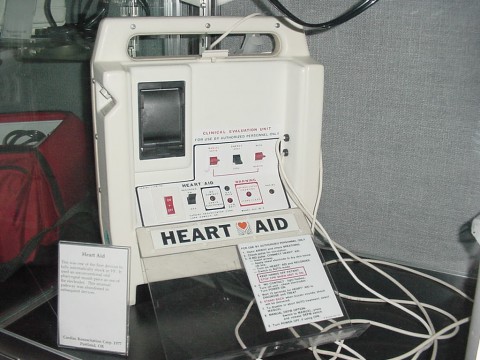
Called the Heart-Aid, the device they developed became the precursor to the modern automated external defibrillator (AED).
The Heart-Aid
The Heart-Aid could be used by bystanders in an emergency to deliver potential lifesaving defibrillation before emergency personnel arrived on scene.
Its operation was based on the familiar ABC approach: airway, breathing, circulation.
An oropharyngeal airway (OPA) was created as one of the two electrodes to deliver the electrical shock. The belief was that a responsive person would gag if an OPA was inserted into their mouth and upper airway, negating the need to go further.
If the OPA was accepted, a small microphone could detect breathing sounds and thus not operate.
To assess circulation a computer chip measured the heart’s electrical activity between the OPA electrode and another electrode contained in a pad attached to the upper abdomen as an independent determination of the need for defibrillation.
The adhesive electrode created a hands-off opportunity to virtually eliminate the potential for accidentally shocking the person operating the device. It is now a standard safety feature on all defibrillators.
The Heart-Aid also paved the way for establishing a feature in which a human voice could talk the user through the device’s operation, also now standard on all AEDs.
A modern precursor
Wayne, who worked at St. Luke’s Hospital and was developing EMS at the time, was acquainted with the inventors of the Heart-Aid AED.
“They put it in a suitcase. It was heavy, like all the early defibrillators were,“ he says. “It had a unique pathway. You pushed the button, and it was ready, set, and go. It also was not biphasic; it was monophasic. It was an interesting solution for the time.
“You approached an unconscious person and attempted to rouse them. If they did not [awaken], you attempted to apply the oral pathway and place the upper abdominal pad. At that point the patient was unconscious, accepting of the airway, and the machine had not locked out. You pushed the go button, and the machine took over on its own—not a lot of warning, and it fired.”
When Wayne first used the AED to respond to a man-down call, he put the device on the patient, and it shocked him.
“This was before Bellingham Fire Department EMS had paramedics, so no standard of care was being violated,“ he says. “There was no local IRB at that time. It worked exactly as it was supposed to.“
Wayne would go on to use it on several more patients, noting its successes and failures.
Several hundred Heart-Aid units were produced by the Cardiac Resuscitator Corp. Although it never gained commercial success, several of its elements are part of the modern AED unit.
Oral pathway pros and cons
Its use of the tongue was a primary reason why the invention as it stood never took off on a widespread basis, says Wayne.
“Further, the concept that the lay public could successfully operate the device was still yet to be achieved,“ he adds. “The idea was, if you had two pads, then you had to figure out where to put them, and what was the lockout? How did you prevent the thing from firing inappropriately? What about pacing, another device feature?
“The idea was, can you put an oral airway in the mouth. The patient has to be able to tolerate the oral airway. Two, the small microphone on the end would sense any airway movement. That meant you couldn‘t be doing CPR while the machine was analyzing. If you use the tongue as a sensoring site, it’s a very good electrical transmitter. It’s going down the musculature of the esophagus.“
The other electrode being a pad applied to the lower chest presented an efficient electrical pathway, adds Wayne. But the idea didn’t garner widespread enthusiasm.
“People don‘t like people shoving things in people‘s mouths,“ Wayne notes. “The general public would be loath to be doing that. They don‘t want to be anywhere near anybody‘s mouth, get bit, get punched. There was too much angst over where they were placing the device.
“They worried about breaking teeth, forcing gags and vomiting—the issues related to an oral pathway. The electrical concept was received. The electrical execution of using it was not well received as people began to try it.“
Still, the Heart-Aid served as a template upon which today’s AED technology is based.
“You don‘t have to be a doctor or nurse or paramedic to use the device. It is fairly simplistic. It did not have much in the way of instructions. It didn‘t have a warning. However, it did have a sound it made when charging,“ Wayne says. “But other than that, you didn‘t have to push a button. It was fully automated. It took a lot of decision-making out of it.“
There were some concerns people would get shocked unnecessarily.
“So fully automated was not the way to go,“ says Wayne. “Later devices became semi-automated. You had to push a button to activate them.
“The other message it sent was, this device is not just for a very select group, but it needs to be in the purview of the public. The third message it sent is that innovation sometimes takes a long time to be accepted. We need to be more open to innovation.“
The start of the story
Wayne would like to see people acknowledge the groundbreaking work of those who set the stage for the modern AED.
“How many AEDs do you see on an average day when you go shopping, to the gym, to the airport, to the hospitals? Who knows how many of those have saved how many lives?
“If you ask any EMT, any paramedic, probably any emergency physician or cardiologist the question of who created the AED and how it was developed, I will bet you 99.9% of the time, they don’t know the answer to that.“
Wayne says although he considers himself to be a “small cog in a big wheel” that produced this innovation, he appreciates it was the beginning of what people now take for granted as they see it on a wall—like a fire extinguisher—in so many common locations.
“Every time I read about an AED saving someone’s life, I think of how kind of cool it was that we were at the start of this story,“ he says.
Carol Brzozowski is a freelance journalist and former daily newspaper reporter in South Florida. Her work has been published in more than 200 media outlets.
SOURCE: EMS World. Reprinted with permission